What Are The Stages Of Diabetic Retinopathy?
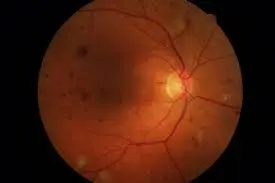
Diabetic retinopathy is a common eye condition caused due to changes in the blood vessels of the retina. The retina is a thin and delicate inner membrane lining the back of the eye. It is a light-sensitive part that helps us see clearly.
The damage to these blood vessels caused due to an increase in the blood glucose levels in patients with diabetes could harm the retina. When these blood vessels become thicker, they develop leaks, which can later lead to vision loss.
The progress of diabetic retinopathy to eventually cause vision loss occurs over a period of time. Hence, for easier understanding, diabetic retinopathy is graded into various stages. The treatment of diabetic retinopathy varies depending on the stages of this condition. If you want to learn more on how to prevent diabetic retinopathy, we did extensive coverage in this post.
Here is a brief discussion about the various stages of diabetic retinopathy and what happens during each of these stages.
Know your risk of diabetic eye disease
Click here to download the RetinaRisk app now!


The 4 Stages of Diabetic Retinopathy
Diabetic retinopathy is a chronic progressive eye disease that is classified into 2 forms and 4 stages.
The 2 types of this condition include non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR).
The term non-proliferative refers to the early stages of this disease, while the term proliferative refers to the more severe changes developed in the retina indicating an advanced form of this disease.
Let us now learn what happens in each of these stages of diabetic retinopathy.
Stage 1: Mild non-proliferative diabetic retinopathy
The first stage of diabetic retinopathy is mild and non-proliferative in nature. It is characterized by a balloon-like swelling in a small area of the wall of the blood capillaries in the retina.
It is the earliest stage of retinopathy, in which tiny areas of swelling develop in the delicate blood vessels of the retina. These small areas of swelling are called micro-aneurysms.
At this stage, a small amount of fluid leaks into the retina, triggering swelling and damage even to the macula, which is a part close to the center or middle part of the retina.
Patients having mild non-proliferative diabetic retinopathy have at least one micro-aneurysm though they usually do not show any other signs of damage to the retina.
Also, the findings are often so subtle that they are not detectable unless examined closely by an expert ophthalmologist. Hence, close inspection and regular monitoring of the eyes and retina are essential for patients with diabetes so that even these subtle changes can be detected before more number of micro-aneurysms develops in the blood vessels.
Patients with mild non-proliferative diabetic retinopathy should ideally have one dilated eye examination of the eyes every year. They have a 5% risk of developing the more severe stages of retinopathy like proliferative diabetic retinopathy within a year.
If more than one micro-aneurysm has developed in the eye of the patient who is not diagnosed with diabetes, they should still be considered to have suspected diabetes and see their primary care physician for further testing.
Detection of the subtle findings and noting the exact locations of micro-aneurysm is essential at this stage to help monitor the progression of the disease. Use of fundus photography, when available, is often recommended in these cases for easier comparison of the changes in the retina in the future.
While the patients with mild NPDR need to be monitored regularly, they do not always need to be referred to a retina specialist. However, it is important that patients are aware of the findings, especially if they are diagnosed with diabetes recently, to ensure they realize that the development of micro-aneurysm indicates early organ damage. They need to be careful and be educated on the possible ramifications of these changes.
Patients should also be encouraged to monitor their blood glucose levels and diet on a regular basis. The results of the blood glucose levels should be shared with the primary care physician, endocrinologist, and ophthalmologist to aid their decision-making related to the treatments.

Stage 2: Moderate non-proliferative diabetic retinopathy
The second stage of diabetic retinopathy is marked by blockages in some of the blood vessels of the retina.
Patients may also have an increase in the swelling in the small blood vessels due to which the blood flow to the retina is compromised. It may affect the nourishment that the retina can receive thus hampering its ability to heal and repair itself.
There is also an increase in the accumulation of fluids and blood in the macula at this stage.
At this stage, the micro-aneurysm that had developed in the first stage of diabetic retinopathy may burst causing hemorrhages in 1 to 3 quadrants of the retina. Other signs indicating the progression of the damage to the retina and macula like cotton wool spots, venous beading, and hard exudates also become evident at this stage.
Patients with moderate NPDR should undergo an eye check-up once in 6 to 8 months.
The risk of PDR within one year is nearly 12% to 27% in patients having the second stage of retinopathy. The use of fundus photography is often recommended for these patients for assessing damage to the retina. The test provides images of the macula that can help in determining the stage of diabetic retinopathy.
These patients do not always need to visit a retina specialist unless the diagnosis of diabetic macular edema is confirmed.
Also, depending on their blood sugar control and the complete diabetes examination by a primary care physician or endocrinologist, it might be necessary to reconsider the changes in the treatment.
Stage 3: Severe non-proliferative retinopathy
The third stage of severe non-proliferative retinopathy is marked by the worsening of the blockages in the blood vessels, due to which some parts of the retina no longer receive an adequate supply of blood.
Without a smooth blood flow, the tissues of the retina can not grow new vessels to replace the damaged vessels in order to restore the supply of oxygen and nutrients. Hence, at this stage, the damage to the retina is likely to progress at a faster rate as the self-repair mechanisms of the affected part of the eye are severely hampered due to the lack of supply of healing nutrients.
Patients with severe non-proliferative retinopathy may also have intraretinal hemorrhages, often more than 20 in each of the quadrants, along with venous beading in at least 2 quadrants. Venous beading refers to the irregular dilatation and constriction of the venules in the retina due to which the symptoms linked to vision loss become worse at a faster speed.
Other than these, the development of other intraretinal microvascular abnormalities (IRMA) can also occur in one or more quadrants of the retina at this stage. IRMA refers to the shunt blood vessels that appear as the abnormal dilation or branching of the existing blood vessels or capillaries in the retina to help supply the areas of lower blood perfusion.
These findings in the absence of the formation of new blood vessels through a process called neovascularization would indicate the patient has already developed the next stage of retinopathy called proliferative diabetic retinopathy (PDR).
Patients diagnosed with severe NPDR need to be monitored more frequently using macular OCT as well as fluorescein angiography for the early detection of macular edema or early neovascularization.
Regular visits to a retina specialist are highly recommended for patients with severe NDPR. They should be monitored once every 3 to 4 months with the dilated fundus examination.
Patients with severe NPDR also have a nearly 52% risk of developing PDR within just 1 year. Hence, it is highly important to be aware of the importance of maintaining proper blood sugar control and regular observation.
The treatment should preferably be planned by a team of healthcare practitioners including the primary care physician, endocrinologist, and ophthalmologist as these patients are at a higher risk of faster disease progression and permanent vision loss. They are also most likely to experience neuropathy in other parts of the body.

Stage 4: Proliferative diabetic retinopathy
The fourth and final stage of diabetic retinopathy is called proliferative retinopathy. It is the most advanced stage of the condition in which additional new blood vessels begin to grow in the retina, though they are abnormal and fragile. Due to this, they tend to leak blood as a result of which patients may develop vision loss and even blindness.
Also, since the newly formed blood vessels are fragile and prone to fluid leakage, patients may also develop other vision problems like blurriness, and reduced field of vision at the early phase of PDR.
Patients with PDR, often exhibit neovascularization in the retina along with vitreous or pre-retinal hemorrhage.
These patients need to visit a retina specialist at the earliest for further tests and treatment. In most cases, peripheral neovascularization is treated with laser pan-retinal photocoagulation along with anti-VEGF intravitreal injections usually performed in combination with PRP (platelet-rich plasma) therapy.
Why is it important to be aware of the different stages of diabetic retinopathy?
The 4 stages of diabetic retinopathy are based on the severity of the damage to the retina and the risk of vision loss. The initial 2 stages of this condition include mild and moderate non-proliferative diabetic retinopathy.
Patients diagnosed with mild non-proliferative diabetic retinopathy usually do not need any active medical intervention by a retina specialist unless the diagnosis is confirmed or if they are concerned about developing a more severe form of an eye disease called diabetic macular edema. Learn all about diabetic macular edema here.
However, in most cases, the risk of developing complications like vision loss is lower at this stage, if proper treatment to control diabetes is initiated.
Patients with moderate non-proliferative diabetic retinopathy have nearly 12 to 27% chances of developing a more severe stage of this condition called proliferative diabetic retinopathy within just one year of the diagnosis. These patients need to visit an ophthalmologist every 6 to 8 months for eye check-ups during which the swelling and damage to the retina are assessed and appropriate treatment is recommended to prevent or slow down the progress of the disease.
Patients with severe non-proliferative diabetic retinopathy have a nearly 52% risk of developing PDR within one year of the diagnosis. These patients are also at a very high risk of faster disease progression and even permanent vision loss. They are likely to experience neuropathies in other parts of the body.
These facts point to the need for regular eye check-ups so that the signs of diabetic retinopathy such as the damage to the vessels and the retina are detected at an earlier stage.
Patients with diabetes are advised to visit their ophthalmologist on a regular basis to assess their eye health so that diabetic retinopathy can be detected at an early stage. Optimum control of your blood sugar levels and seeking early treatment of complications like diabetic retinopathy is the key to protecting yourself against the possible impairment of vision.
Treatment of diabetic retinopathy
Patients with diabetic retinopathy are usually treated with focal laser photocoagulation of the macula and the intravitreal injections of medications called anti-VEGF agents. However, laser treatment may not be suitable for all patients as it may cause more scarring and permanent loss of vision. Hence, the intravitreal administration of anti-VEGF agents is often the first line of treatment for most patients with diabetic retinopathy. We have covered the treatment of diabetic retinopathy here in detail.

Conclusion
Diabetic retinopathy is one of the common complications of diabetes caused due to the damage to the back of the eye called the retina as a result of the high blood glucose levels. If left undiagnosed and untreated, it may cause partial or complete loss of vision. A late diagnosis of diabetic retinopathy could also make the treatments less effective and even lead to permanent blindness.
It often takes several years for the changes in the retina to become worse and reach a stage where it threatens your eyesight. However, the damage to the retina is not completely reversible.
The best outcomes for the treatment of diabetic retinopathy are obtained when it is diagnosed in the initial stages. Hence, controlling your blood sugar levels and having routine eye check-ups are highly recommended for protecting your eyesight.